Aspergillosis infections in birds of prey
A. A. Oranje, DVM and R. M. Gerrits, DVM
Topet Farma BV, Abbinkdijk 1, 7255 LX Hengelo, Netherlands. E-mail: info@topet.nl
Introduction
The subject of this article is infection with Aspergillus in birds of prey. The disease caused by Aspergillus is called aspergillosis. Aspergillosis is the most common infectious disease found in captive birds of prey.
The disease is mainly caused by Aspergillus fumigatus, but other fungi of the same genus, such as Aspergil/us flavus and Aspergil /us niger also cause this disease incidentally. The most common location in which aspergillosis is found is the respiratory tract.
Aspergil/us is a fungus. It grows in environments rich in oxygen. Aspergillus grows by forming hyphae; these are threadlike structures which cover surfaces. When ready for reproduction, spores are formed. Spores are very small particles of infectious material. They detach, become airborne and are capable of contaminating the environment.
Inhalation of the airborne spores is the principal mode of transmission. Aspergillus spores adhere to the mucosa I linings of the respiratory tract and start multiplying. Next to the space invading properties and covering of mucosa I surfaces, there is additional pathogenic activity from the toxin producing strains. Some toxins produced by Aspergillus are known to suppress the immune system of the bird. This predisposes the patient to other conditions. Also, toxins can evoke allergic-like reactions, causing acute respiratory distress.
Some species of birds of prey appear to be particularly susceptible to aspergillosis, among them Goshawks Accipiter gentilis, Gyrfalcons Falco rusticolus, Red-tailed Hawks Buteo jamaicencis and Snowy Owls Nyctea scandiaca.
Whether or not a bird gets clinically ill after coming into contact with Aspergillus depends on different factors. Aspergillosis is often seen as a secondary disease. This means it arises more easily when a stressor or condition is present, affecting the health of the bird. These stressors can be present in the birds or its environment and compromise the immune system. A stressor can be for example: travel (death caused by Aspergillus infection is an important problem in the import and export of birds), nutritional deficiencies, cutting back the offered food load, concurrent disease and/or trauma.
Another factor contributing to the development of the disease is the pathogen load. An environment high in Aspergillus spores promotes the development of aspergillosis.
Aspergillosis
After inhalation of Aspergillus spores, disease can develop following different pathologies. Because of the unique anatomy of birds, spores can adhere to the mucosal wall of trachea, bronchi, air sacs and to the lungs. This doesn't always cause disease. The immune system of a healthy bird can prevent spores from causing disease after they are inhaled. Problems arise when the immune system isn't capable of neutralizing the spores. A large burden of spores is sometimes too much for the immune system to eliminate, even in healthy birds. In these cases the spores can adhere, flourish and grow into fungal colonies.
Aspergillus spores can develop into large granulomas. These are masses of hyphae and infected tissue. These cause problems because of their space invading qualities. Additionally, they are a constant source of new spores, causing contamination of the environment and also causing a more extensive spread in the body of the infected bird.
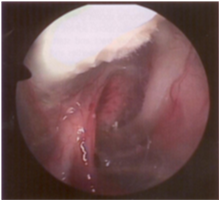
Picture 1. shows a large granuloma in an airsac. The spore forming hyphae give the granuloma a ‘fluffy’ appearance.
In other patients the lesions are more dispersed through the body and consist of smaller masses of Aspergillus. An example of a more diffuse manifestation of Aspergillosis is shown in Picture 2.
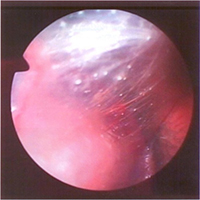
Picture 2. small foci of fungal growth are visible on the airsac.
Acute aspergillosis
The acute form of aspergillosis is often teen affer inhalation of a large number of spores, cortibined with a compromised immune system. Most commonly affected in this pathology are the lungs, which exhibit many small granulomas throughout the lung tissue. This causes acute respiratory distress and often leads to the death of the patient. Especially in toxin producing strains of Aspergil /us, the disease can have a very short course before leading to the death of the bird.
Chronic aspergillosis
More often c;spergillosis presents itself as a chronic condition: It often takes weeks to months to cause visible signs of disease. Usually the first signs to be noticed are unspecific and consist of weight loss and a loss of performance in flight. The birds may exhibit subtle changes in behaviour and have a reduced appetite. In the next phase of the disease more prominent signs may become visible, such as dyspnoea, a change of voice. Further clinical signs will depend on the location of the Aspergillus in the body.
Early in the disease granulomas often arise in the trachea, bronchi, lungs and air sacs. Because of the unique anatomy of birds, and the lack of a diaphragm, infections in the respiratory tract can spread easily to other parts ofthe body, including the abdominal organs. Depending on the severity of the lesions, different clinical signs can present themselves. Examples of organs commonly affected are the ovary and testis; this can result in poor breeding. In case of involvement of the kidneys, polyuria, polydipsia and gout may be observed.
An acute deterioration of the condition of the bird suffering from the chronic form of aspergillosis is in the occurrence of a granuloma in the trachea. Sometimes parts of these granulomas tear off and can get lodged in the trachea, on the syrinx or in one of the main bronchi. This leads to very acute, severe respiratory distress and can even result in suffocation and death.
Diagnosis
There are several diagnostic methods to diagnose aspergillosis.
Haematology and biochemistry/bloodwork
This can be useful to determine the condition of the birds and it also can give an indication about the presence of a fungal infection. In case of aspergillosis the results will often indicate a chronic inflammatory process. The white blood cell count is often high (white blood cells are important cells to the immune system, their numbers are elevated in case of increased need, as is the case in infections). This elevated level of white blood cells is often caused by elevated heterophils (a special kind of white blood cell), sometimes these exhibit abnormal shap -or contents which further suggest the presence of aspergillosis. In case of aspergillosis which also involves liver and kidneys (as is usually the case in chronic aspergillosis), the values providing information about these organs are also elevated (UA, ALT, AST, GGT). Globulin and Total Protein in the blood are often elevated (indicating infection), and several minerals are found to be present in the blood in higher concentrations than usual (Iron, Calcium, Phosphate). This could possibly be caused by impaired liver function due to the Aspergillus infection. Unfortunat ly, all these changes could also be anributat!fe to other chronic inflammatory processes. Therefore mere blood work does not suffice to diagnose a bird with aspergillosis, but aids in the diagnosis and gives an indication of the overall severity of the condition.
Radiographs
Radiography can be useful in the diagnosis of aspergillosis. It is not a very sensitive method and lesions tend to be quite extensive before becoming visible on radiographs. Usually Aspergillus lesions are visible as distinct nodular lesions. Since other pathologies may cause similar images, caution should be taken with the interpretation of these radiographs. Also, sometimes a severely affected bird will exhibit no abnormality on radiographs.
Endoscopy
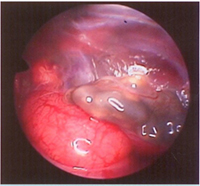
Because the anatomy of birds allows with relatively minimal invasiveness to directly examine the inside of the bird, this is a very useful method to directly visualize a lot of problems. By entering the most abdominal air sac, the mucosa of the air sacs can be inspected, the internal organs including the lungs can be visually examined and biopsies can be obtained for further diagnostic procedures. In cases of well-developed granulomas, diagnosis can usually be confirmed during the endoscopic procedure. In case of more indistinct lesions, biopsies can be obtained from the suspected lesions.
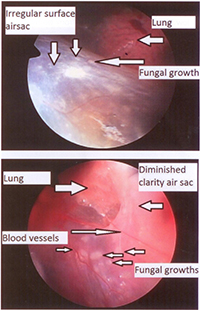
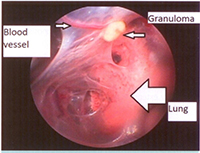
Pictures 3, 4 and 5 (above) show different photographs taken during endoscopic examination. They show the different manifestations of aspergi!losis. Pictures 3 and 4 are pictures of a bird with a widespread form of aspergillosis with small lesions on the airsacs. Picture 5 is a more localized form of aspergillosis, with distinct granulomas.
Microscopy / Culture
In case of Aspergillus granulomas in the trachea, a tracheal swab can be examined microscopically and the fungal hyphae can be visibly determined .The diagnosis can be confirmed by culturing the material from the swab on a specialised plate and incubating until fungal growth is visible.
Since Aspergillus can be found in the environment in low numbers, trachea l swabs from both affected and healthy birds may yield Aspergillus on culture. It is therefore advisable to always examine the swabs under the microscope to identify hyphal structures, after performing the collection of material. Hyphae indicate a growing fungus and are a more sound evidence of the presence of an active infection. Biopsies taken during endoscopy can be examined in a similar manner.
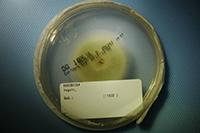
Picture 6 shows fungal growth on this plate. The material in thecentre of the fungal growth is a biopsy of a suspicious lesion in an airsac. It was taken during endoscopic examination.
For diagnosis of Aspergi llus infection in birds of prey, combining diagnostic techniques is recommended to diminish the chances of an incorrect diagnosis and to have a complete picture of the overall health of the bird.
Treatment
Over the years several treatments have been developed for aspergillosis in birds of prey. Since the disease is often fairly extensive, treatment can be a challenging and long-term process.
Antifungal drugs are used to eliminate the fungus. There are different groups of medicines, each with their own mode of action. Also there is a variety in ways of administration of these different drugs.
Until recently there was a vast lack of medicine research in birds. No registered products especially for birds intended to treat funga l infections were available.
Oral administration
Nystatin and amphotericin 8 are polylene antimycotics and bind to ergosterol within the cell wall of the fungus. This creates a hole in the cell wall, which causes the degradation of the fungus. These drugs are not absorbed after oral administration . Therefore they are effective in treating fungal infections of the mouth and intestinal lumen, but won't reach effective concentrations in other tissues. Given as oral medicine it has thus limited use in the treatment of aspergil losis in birds of prey.
Another group of antifungal medicines are the azoles. The best known member of this group is itraconazole. ltraconazole inhibits the synthesis of ergosterol (an important component of the fungal cell wall). It also affects membrane permeability, resulting in structural degeneration of the fungus. ltraconazole is thereby a medicine with an activity wh ich consists of stopping the expans ion of the fungus, but it wil l also diminish the lifespan of the fungus.
Using a product which has not been testeti on birds, can have unexpected side effects, due td differences in excipients, which can influence bioavailability.
Unfortunately, very few well researched, registered avian medicines are currently available.
In March 2014, an antifungal medicine was authorized in Europe specifically designed for the treatment of fungal infections in birds. Fungitraxxs is a solution containing itraconazole. During the registration procedure a large field study was conducted, with very favourable results. Next to the ac;tive ingredient (itraconazole), Fungitraxxs contains a tiigh dose of cyclodextrin. This is a sugar molecule which envelops the itraconazole molecule. This improves absorption by the intestines and thereby enhances bioavailability. This is possibly a contributing factor to the high rate of full cure seen with the use of Fungitraxx®.
In Red-Tailed Hawks itraconazole has been found to be safe. Effective blood and tissue levels have been reached by once a day dosing of 10 mg per kilogram body weight (this is the same dose as used in the Fungitraxx® field study).
ltraconazole has good effectivity and few side effects. Most of the side effects are dose related and consist of nausea and vomiting. These side effects are reversible when lowering the dose.
Long-term treatment is often necessary because of the extensive spread of the fungal infection, and of the indirect mode of action of the antifungal drugs.
Nebulisation
Different medications are used by nebulization. With this method it is a necessity to provide droplets smaller than 3 micrometres to reach the lungs and air sacs. Larger particles will be deposited onto nasal and oropharyngeal mucosa! surfaces and in the trachea, and won't reach the lower airways. Used as sole treatment, nebulisation is unlikely to provide a full cure, since most cases of aspergillosis have spread to several internal organs next to the respiratory tract. Medication administered by nebulisation will not penetrate large granulomas deep enough to cause significant damage to the fungal growth.
Next to the known antifungal drugs a product called FlO is used with apparent beneficial effect. This product contains Benzalkolium Chloride and Polyhexanide, these are antiseptic agents which damage the fungal cell wall. Unfortunately, very few studies have been conducted to examine the clinical effectivity of this product in treating avian Aspergi /lus infections.
Nebulisation of medications can be used as a complementary thera py inthe treatment ofaspergi llosis.
Intravenous administration
Amphotericin B can be used as an intravenous drug.This is an antifungal drug with a cidal action, meaning it kills the fungus. There have been seen serious side effects after administration of this drug. This, combined with the inconvenience of repeated intravenous injections, is a severe disadvantage as a therapy for aspergillosis in avian patients.
Surgery
In case of large granulomas, especially located in trachea or syrinx, surgical removal can be helpful in curing the bird. Large granulomas in air sacs can be partially removed by endoscopy, contributing to better penetration of antifungal drugs. It will however always be necessary to have a surgical procedure be followed by treatment with systemic antifungal drugs.
Prognosis
In case of acute aspergillosis the prognosis is usually very poor. Chronic aspergillosis can be cured completely, but may take a very long time. Especially in case of large granulomas, oral administration of antifungal drugs may need to be administered 6-8 months. Repeated endoscopic inspections are paramount to track the development of the disease, and to prevent premature cessation of therapy.
Picture 8 shows on encapsulated gronulomo in the air soc. Lesions like these ore very difficult to reach by ontifungol drugs, and these lesions will toke a long time to be completely resolved.
Prevention
Aspergillosis is found in captive birds of prey in larger incidence than reported in their wild congeners. There may be several factors contributing to this difference. Spore load in the environment is likely to be more prominent in an enclosure than in the natural environment of wild birds. Especially damp bedding and/or nests may contain large numbers of fungal spores (and other pathogens such as bacteria, moulds and parasites). Therefore, in the prevention of aspergillosis it is extremely important to have good hygienic protocols. There are several cleaning products on the market which will eliminate Aspergi /lus spores. Care should be taken when treating the enclosures to make sure the disinfectants pose no threat to the birds.
Another factor contributing to the development of aspergillosis in captive birds of prey are external stressors that compromise immune function. Aspergillosis is often seen in birds after a period of travel, it is one of the main illnesses seen in newly imported or exported birds. Also, the period prior to the hunting season, when birds of prey are forced to lose weight, is a known stressor that increases the chances of developing aspergillosis.
Vitamin deficiencies, especially vitamin A, is suspected to cause a higher sensitivity to respiratory infections. Vitamin A is needed for optimal mucosal integrity, deficiencies of this vitamin are likely to diminish the natural defence strategies of the mucosa. Optimal nutrition is therefore very important in preventing Aspergillus infections.
When confronted with a less than optimal situation and/or events, such as a parasite load, traumatic injuries, and others, vigilance is needed to prevent concurrent aspergillosis to develop.
Corticosteroids are pharmaceuticals that dramatical ly compromise immune function and should be used in birds only with the utmost care, and preferably be avoided altogether.
There have been some studies about vaccination against Aspergillus, but so far no vaccination for practical use is available. Further studies are needed to determine the value of this form of preventive medicine.
Prophylactic treatment with antifungal drugs is suggested to have beneficial effects in diminishing the chances of developing aspergillosis. This could be used in periods known to compromise immune function.
References
Cooper JE. 2002. Birds of Prey: Health and Disease 3rd Ed. Wernery R et al. 2004. Colour Atlas of Falcon Medicine. Harrison et al. 2006. Clinical Avian Medicine.
Hsu. 2013. Handbook of Veterinary Pharmacology
Jones MP et al. 2000. Pharmacokinetic disposition of ltraconazole in Red-Tailed Hawks (Buteo jamaicensis). Journal of Avian Medicine and Surgery 14: 15-22.